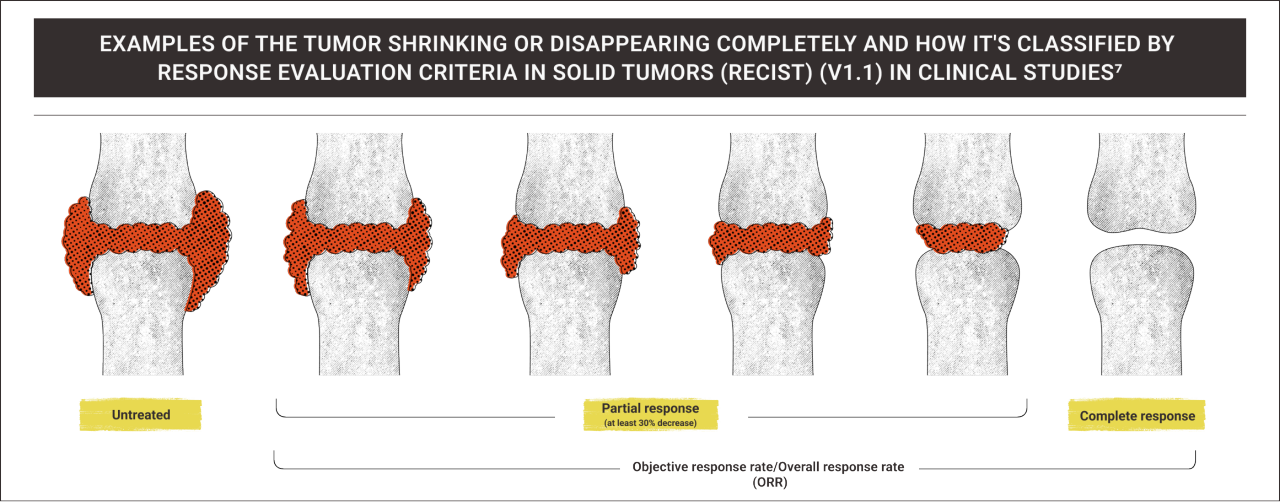
1. TGCT Support. Clinical trials. Updated 2025. Accessed March 4, 2026. https://www.tgctsupport.org/clinical-trials.html. 2. Stacchiotti S, Dürr HR, Schaefer IM, et al. Best clinical management of tenosynovial giant cell tumour (TGCT): a consensus paper from the community of experts. Cancer Treat Rev. 2023;112:102491. doi:10.1016/j.ctrv.2022.102491. 3. Gelhorn HL, Tong S, McQuarrie K, et al. Patient-reported symptoms of tenosynovial giant cell tumors. Clin Ther. 2016;38(4):778-793. doi:10.1016/j.clinthera.2016.03.008. 4. National Comprehensive Cancer Network. Why should I consider a clinical trial? Accessed March 4, 2026. https://www.nccn.org/docs/default-source/patient-resources/clinical-trials/download-a-printable-handout-to-learn-more-about-clinical-trials.pdf. 5. US Food and Drug Administration. Step 3: clinical research. Accessed March 4, 2026. https://www.fda.gov/patients/drug-development-process/step-3-clinical-research. 6. National Institutes of Health. Glossary of Common Terms. Accessed March 4, 2026. https://www.nih.gov/health-information/nih-clinical-research-trials-you/glossary-common-terms. 7. Villaruz LC, Socinski MA. The clinical viewpoint: definitions, limitations of RECIST, practical considerations of measurement. Clin Cancer Res. 2013;19(10):2629-2636. doi:10.1158/1078-0432.CCR-12-2935. 8. Goldmacher GV, Conklin J. The use of tumour volumetrics to assess response to therapy in anticancer clinical trials. Br J Clin Pharmacol. 2012;73(6):846-854. doi:10.1111/j.1365-2125.2012.04179.x. 9. Ruchalski K, Braschi-Amirfarzan M, Douek M, et al. A primer on RECIST 1.1 for oncologic imaging in clinical drug trials. Radiol lmaging Cancer. 2021;3(3):e210008. doi:10.1148/rycan.2021210008. 10. National Cancer Institute. Tumor volume. Accessed March 6, 2026. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/tumor-volume. 11. Peterfy C, Chen Y, Countryman P, et al. CSF1 receptor inhibition of tenosynovial giant cell tumor using novel disease-specific MRI measures of tumor burden. Future Oncol. 2022;18(12):1449-1459. doi:10.2217/fon-2021-143. 12. Shahid A, Wilkinson K, Marcu S, Shapiro CM, eds. STOP, THAT and One Hundred Other Sleep Scales. Springer; 2012. 13. Speck RM, Ye X, Bernthal NM, Gelhorn HL. Psychometric properties of a custom Patient-Reported Outcomes Measurement Information System (PROMIS) physical function short form and worst stiffness numeric rating scale in tenosynovial giant cell tumors. J Patient Rep Outcomes. 2020;4(1):61. doi:10.1186/s41687-020-00217-6. 14. Shelbourne KD, Biggs A, Gray T. Deconditioned knee: the effectiveness of a rehabilitation program that restores normal knee motion to improve symptoms and function. N Am J Sports Phys Ther. 2007;2(2):81-89. 15. Gandbhir VN, Cunha B. Goniometer. In: StatPearls. Treasure Island (FL): StatPearls Publishing; June 7, 2020. 16. Stern S, McKenzie PF, Bernthal N, et al. Localized and diffuse tenosynovial giant cell tumor: real-world results from a patient observational registry. Future Oncol. 2025;21(12):1501-1510. doi:10.1080/14796694.2025.2488635. 17. Jensen RE, Potosky AL, Reeve BB, et al. Validation of the PROMIS physical function measures in a diverse US population-based cohort of cancer patients. Qual Life Res. 2015;24(10):2333-2344. doi:10.1007/s11136-015-0992-9.
18. Palmerini E, Trent JC, Hornicek FJ. Medical management of tenosynovial giant cell tumor. Curr Oncol Rep. 2025;27:844-855. doi:10.1007/s11912-025-01679-x. 19. National Cancer Institute. CTCAE and adverse event reporting. Accessed March 4, 2026. https://dctd.cancer.gov/research/ctep-trials/for-sites/adverse-events. 20. Christensen AMM, Dowler K, Doron S. Surgical site infection metrics: dissecting the differences between the National Health and Safety Network and the National Surgical Quality Improvement Program. Antimicrob Steward Healthc Epidemiol. 2021;1(1):e16. doi:10.1017/ash.2021.176. 21. Bali RK. Operating room protocols and infection control. In: Bali RK, Kumar P, Sharma V, eds. Oral and Maxillofacial Surgery for the Clinician. Springer; 2020;173-194. 22. Tobin EH, Zahra F. Nosocomial infections. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 2, 2025. 23. Roshanov PS. Bleeding independently associated with mortality after noncardiac surgery (BIMS): an international prospective cohort study establishing diagnostic criteria and prognostic importance. Br J Anaesth. 2021;126(1):163-171. doi:10.1016/j.bja.2020.06.051. 24. Halme ALE, Roshanov PS, Tornberg SV, et al. Timing of major postoperative bleeding among patients undergoing surgery. JAMA Netw Open. 2024;7(4):e244581. doi:10.1001/jamanetworkopen.2024.4581. 25. Spierenburg G, van der Heijden L, Mastboom MJL, et al. Surgical management of 144 diffuse-type TGCT patients in a single institution: a 20-year cohort study. J Surg Oncol. 2022;126(6):1087-1095. doi:10.1002/jso.26991